Author: Masamichi Takono
Coronary angioscopy (CAS) provides morphological information on atherosclerotic plaque, thrombus, and vascular healing after stent implantation. However, adequate observation by CAS requires balloon occlusion and a larger than 6 Fr compatible guiding catheter for complete replacement of coronary blood with transparent fluid. The invasive nature and complexity of the procedures limit the wide utilisation of this imaging device. Herein, we present a novel method of CAS using a slender fibrescope catheter.
A 78-year-old female with stable angina pectoris received coronary angiography (CAG) via the right radial artery. Focal stenosis was found in the proximal right coronary artery, and catheter intervention was performed using a 4 Fr Judkins Right guiding catheter (Kiwami™; Terumo Corp., Tokyo, Japan). We attempted to observe the target lesion using a new type of slender fibrescope (Smart-i™ type S11; iHeart Medical Co., Ltd, Tokyo, Japan). The tip of the catheter traversed the lesion along a 0.014 inch guidewire, and a manual pullback image of CAS was recorded during continuous infusion of contrast media by autoinjector (4 mL/sec, total 12 mL) (Figure 1, Moving image 1, Moving image 2). After implantation of a drug-eluting stent (Resolute Integrity™ 2.75/12 mm; Medtronic, Minneapolis, MN, USA), the lumen was visualised using the same method (Figure 2, Moving image 3).
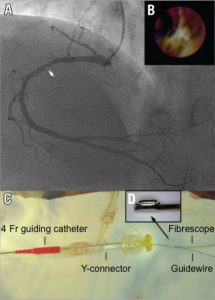
Figure 1. Angiographic and angioscopic findings at baseline and image of the catheter system. A) Coronary angiography showed the culprit lesion in a case of angina pectoris (arrow) in the proximal right coronary artery (RCA). B) Yellow plaque and mural red thrombi were recognised by coronary angioscopy (CAS). C & D) A short monorail type of fibrescope was advanced along a 0.014 inch guidewire through a 4 Fr guiding catheter.
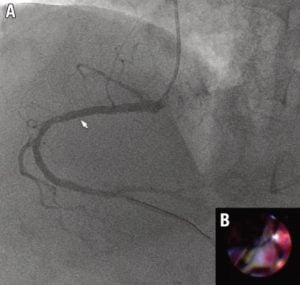
Figure 2. Angiographic and angioscopic findings after coronary intervention. A) Stenosis of the RCA completely disappeared after stent implantation (arrow). B) CAS showed the attachment of the implanted stent to the vessel wall.
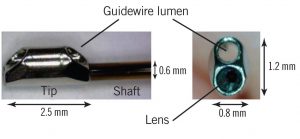
Figure 3. The tip of the angioscopic catheter. The rigid tip (0.8/1.2 mm in diameter) has an object lens and guidewire lumen, and the flexible shaft (0.6 mm in diameter) contains 3,000 pixels of optical fibres. The length of the tip is 2.5 mm, and this postion serves as a radiopaque marker and monorail port.
Supplementary data
[/custom_font]
Moving image 1. Fluoroscopic during angioscopic observation. The tip of the angioscopic catheter was slowly moved from distal to proximal to the target lesion during flushing of contrast media.
Moving image 2. Angioscopic image at baseline. CAS revealed the presence of atherosclerotic yellow plaque and mural red thrombi in the culprit lesion.
Moving image 3. Angioscopic image after stent implantation. Stent struts adequately attached to the plaque and thrombi. Angioscopic observation provided satisfactory image quality for quantitative evaluation of the coronary lumen.