A 93-year-old female started to experience dyspnoea. One month later, she was transported to our hospital due to worsening of the symptom and examined. She was haemodynamically stable, and a slight ST depression was seen in leads V3-6 on an electrocardiogram (ECG). A contrast computed tomography (CT) scan revealed a giant right coronary artery aneurysm (CAA; 28 mm x 34 mm) and pericardial effusion, but ongoing extravasation was not apparent (Figure 1A). We tried to carry out a pericardiocentesis; however, the coagulum made it impossible to aspirate the effusion even though the needle tip was seen within the effusion under fluoroscopy. A coronary angiography (CAG) showed a giant saccular aneurysm in the proximal right coronary artery, though the neck of the aneurysm and its width were difficult to identify angiographically (Figure 1B, Moving image 1). We first thought the best treatment was surgical, that is, resection of the aneurysm with coronary artery bypass grafting and removal of the haemorrhagic pericardial effusion. The feasibility of surgical treatment was discussed by the Heart Team, but it was considered high risk because of the patient’s old age and frailty; thus, we decided to treat it by percutaneous coronary intervention (PCI). We were able to identify the length of the aneurysm’s neck with intravascular ultrasound (IVUS) (Moving image 2). First, we deployed a coronary covered stent (GRAFTMASTER RX 2.8/19 mm [Abbott]) in an attempt to cover the neck; however, the aneurysm was still visible in the subsequent angiography. We then deployed a second covered coronary stent (PK Papyrus 3.5/15 mm [BIOTRONIK]) that proximally overlapped the first stent. Consequently, a complete obliteration of the aneurysm was obtained (Figure 1C, Moving image 3). A contrast CT scan after covered stent implantation showed a sealed aneurysm (Figure 1D). The coagulated pericardial effusion slowly resolved in the subsequent serial CT scans.
A CAA usually remains unnoticed until complications develop, or is sometimes found incidentally by CAG or CT angiography. The right coronary artery is most commonly affected. There is no consensus on the management of CAA, and the treatment is individually tailored in each clinical setting due to the absence of randomised trials and societal recommendations. The current recommendations are based on case studies or anecdotal data12. Successful treatment of CAA using covered stents has been described in several case reports and case studies. The use of covered stents in the treatment of CAA, at least in an elective setting, appears to be both effective and reasonably safe3.
In this patient we successfully treated a giant CAA with a long neck using covered coronary stents. We were able to visualise the neck of the aneurysm with IVUS.
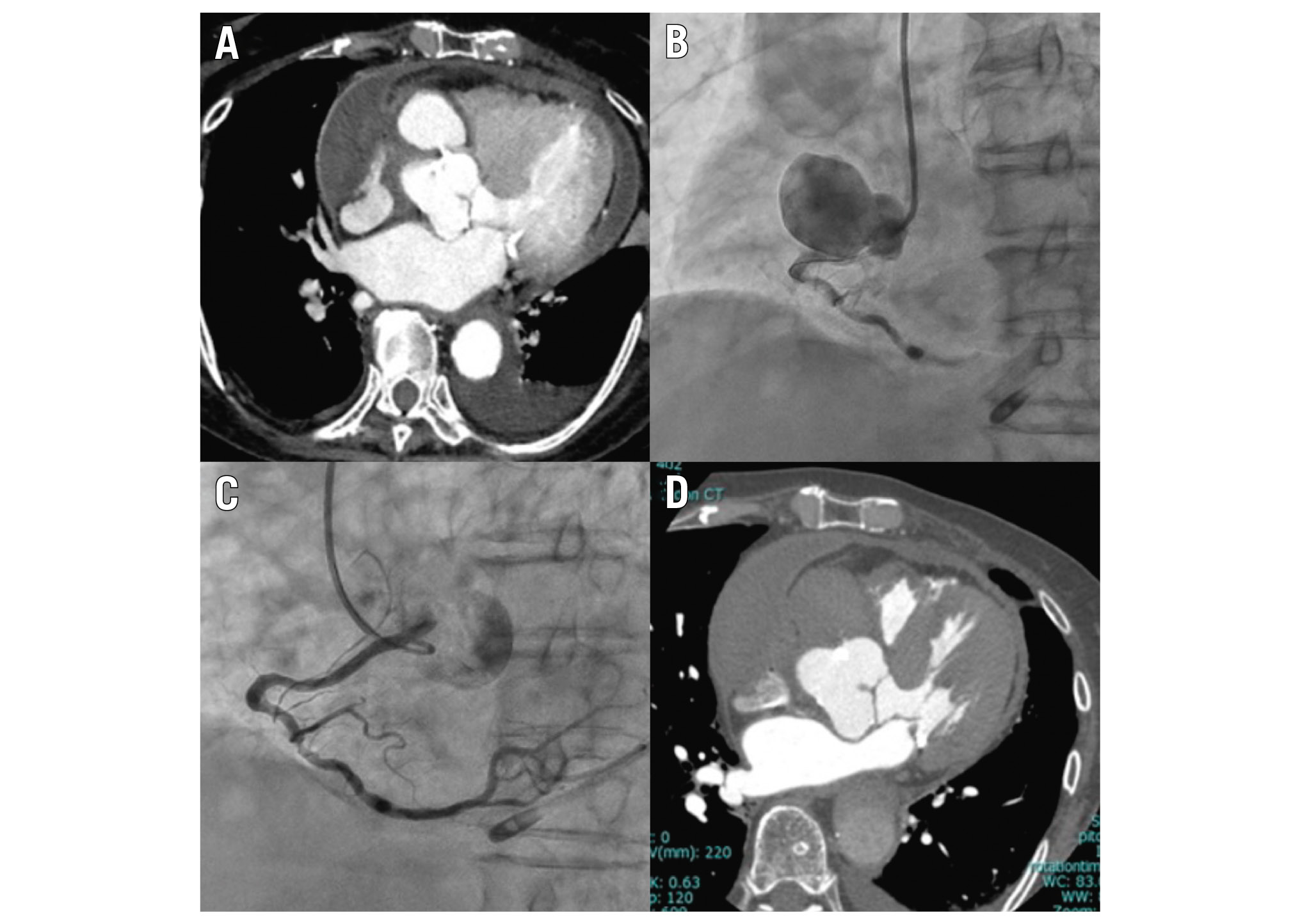
Figure 1. CT images of before and after PCI, and angiogram during PCI. A) Contrast CT scan on arrival. B) Initial angiogram. C) Final angiogram. D) Contrast CT scan after covered stent implantation. CT: computed tomography; PCI: percutaneous coronary intervention
Conflict of interest statement
The authors have no conflicts of interest to declare.
