Huay Cheem Tan1,2*, MBBS, M MEd (Int Med), FRCP (UK), FAMS, FACC, FSCAI, FAPSIC, President of Asian Pacific Society of Interventional Cardiology (APSIC) and Chief Editor AsiaIntervention
AsiaIntervention 2019;5:112-114, DOI: 10.4244/AIJV5I2A19
1. Department of Cardiology, National University Heart Centre, Singapore, Singapore; 2. Department of Medicine, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
The 21st century is commonly dubbed the “Asian Century” because of the robust economic performance and projected demographic growth in this region, with the population expected to increase from the present day four billion to five billion people by 2050. The major driver is productivity growth as living standards rise. The same parallel can be observed in the field of endovascular therapy in the last three decades, with expected phenomenal growth in interventional volume, coupled with research and innovation and widespread upskilling and training of cardiologists in the region.
I entered the field of interventional cardiology and completed my fellowship training in the mid 1990s. I have had the opportunity to witness the development of interventional therapy in the region. There is no question about the explosive growth in the number of coronary intervention cases in Asia driven by double digit growth in China and India. From a mere 12,000 cases in 2000, China performed more than 915,000 in 2018. India has also witnessed rapid growth from 67,000 in 2010 to more than an estimated 550,000 cases performed last year (Figure 1). Considering that both of these (Asia’s two largest countries) have populations that are three times larger than the USA, it is not difficult to imagine that they will exceed the estimated annual 950,000 cases performed in the USA in no time. There have also been many governmental policies formulated in recent years to fund the therapy such as the heavy subsidies for primary percutaneous coronary intervention (PPCI) in Indonesia and Vietnam. It is no wonder that all the major companies in the industry are relooking their marketing and investment strategies in the East.
One has to acknowledge that the Western world has clearly taken the lead in pioneering the technique of coronary angioplasty, from the landmark work performed by Dr Andreas Gruntzig in 1997, to the development of the Palmaz-Schatz coronary stent by Drs Julio Palmaz and Richard Schatz, to the first-inman transcatheter aortic valve implantation in 2002 by Dr Alain Cribier. These achievements have set the stage for future generations of interventionists to build on, many of whom hail from the Asian region.
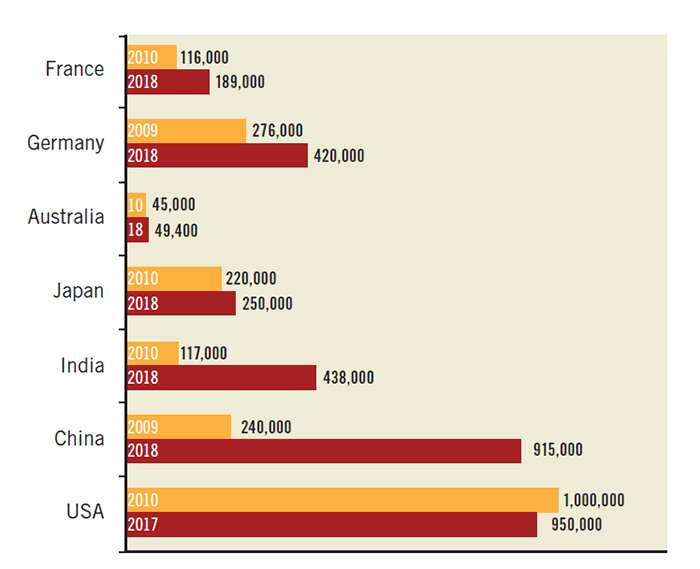
Figure 1. Number of PCI procedures performed around the world.
Following Dr Ferdinand Kiemeneij’s first introduction of transradial access to angioplasty and stent procedure in 1992, there was an almost immediate adoption of this technique in Asia because of the advantage of reducing periprocedural bleeds.
Dr Shigeru Saito started the Yokohama Transradial Intervention Course in Japan; Dr Tejas Patel has written a book on the techniques which has benefited generations of interventionists. In terms of pushing forward new boundaries and techniques, Dr Seung-Jung Park from Korea has shown that PCI of treacherous left main territory disease was feasible and safe, Dr Shao- Liang Chen from China developed the superior technique of double-kissing crush (DK crush) for the treatment of distal left main bifurcation lesions and Dr Osamu Katoh from Japan pioneered the now-common techniques of controlled antegrade and retrograde tracking (CART) and reverse CART for retrograde recanalisation of chronic total occlusion of coronary arteries. In terms of innovation, we remember that it was the late Dr Hideo Tamai from Japan who developed the first bioresorbable scaffold called the Igaki-Tamai stent in 2001, with its interesting self-expanding design using the poly-L-lactic acid polymer. Multivessel complex PCI in high-risk patients, now termed CHIP (complex high-risk indicated patients), with sophisticated and often ingenious techniques are commonplace in Asian countries. This is perhaps a result of the cultural reluctance to undergo open chest surgery among East Asians, with a resultant PCI to coronary artery bypass surgery (CABG) ratio varying from 3 to 100:1. In addition, CABG is not routinely available in most hospitals in Asia and PCI has become the only coronary revascularisation modality available.
While the level of technical expertise has improved considerably over the years, there is still room for improvement in terms of the adoption of an evidence-based approach to PCI. This would include appropriate use criteria, guideline-directed approaches, more use of imaging and physiology-guided therapies, as well as adjuvant pharmacologic therapies. There should also be the systematic training of young fellows, from acquiring core curriculum knowledge, the use of simulator-based technical training, to apprentice-based clinical training with more personal and interactive learning with mentors. There is also a place for better design of clinical trials that are relevant to our practice in Asia. These are areas where I think the Asia Pacific Society of Interventional Cardiology (APSIC) can play a part.
I have been fortunate to be the President of APSIC for an unprecedented two terms of six years’ duration. I have had the opportunity to contribute to the growth and development of endovascular therapy in this vast region. APSIC was officially formed during the 3rd live demonstration course held in Singapore in July 1993. Founded initially by 11 eminent cardiologists who were convinced that the 21st century of growth in interventional cardiology would be in Asia, the group had the vision then to provide a forum in which Asia-Pacific experts could share knowledge and expertise in the field of catheter-based therapies, and to develop joint academic research and education programmes (Figure 2). Membership enrolment for APSIC was to be conducted through the national cardiac societies. It would be under the umbrella of the Asian-Pacific Society of Cardiology (APSC) and the President would be a member of the APSC Council. Drs Richard Ng and Arthur Tan were elected to be the first President and Secretary General of APSIC, respectively. An APSIC newsletter was first published on 29 September 1993 to feature regular updates of scientific development and to share interesting cases and literature reviews among the interventional cardiology fraternity.
In the ensuing 20 years, APSIC has gone through ups and downs but has recently taken on a new momentum. It now boasts membership from 20 Asian-Pacific countries, with 273 fully fledged fellows, including members from Australia and New Zealand, and the Gulf States such as Saudi Arabia and Kuwait. It has a permanent secretariat based in Hong Kong.
Under the current APSIC Board, the Society endeavours to embark on two broad initiatives. The first is to promote the standard of catheter-based therapies in the region through scientific and training activities, and to connect with the rest of the world through collaborative educational opportunities. The Society has its own official scientific meeting called Asian Interventional Cardiovascular Therapeutics (AICT), which is held annually in different AP countries. From 2019 onwards, APSIC will join with the larger PCR family to form the AICT-AsiaPCR meeting. This meeting will incorporate Asian technical expertise with the innovative and educational strengths of PCR to become a true Asian flagship educational meeting. The inaugural meeting will be held in Singapore from 4 to 6 July 2019 and has already generated tremendous support and enthusiasm throughout the entire region, with the expected participation of more than 250 local and international faculties, 2,500 delegates, 300 abstract and case presenters, six Asian national societies and many industry partners. There will be live transmission cases from the National University Heart Centre, Singapore (NUHCS), National Taiwan University Hospital, Taipei, and Clinique Pasteur in Toulouse, France. The meeting will be rotated around selected AP countries every other year, with Singapore selected as its base site.

Figure 2. Founding members of APSIC in Sydney 1993.
Given the increasing flurry of research publications and trials originating from Asia, particularly from Korea, China and India, the second initiative of APSIC is to promote collaborative research activities among member countries, and to synergise the strengths, resources and know-how of the Asia Pacific region as a common entity. The APSIC Research Committee, ably led by Dr Michael Lee from Queen Elizabeth Hospital, Hong Kong, has started the first initiative of the Asia Pacific Transcatheter Aortic Valve Implantation (APTAVI) Registry, which is supported by 10 centres from eight countries. The framework of collaboration is developed based on criteria such as the analyses of outcomes, cost-effectiveness, and quality of care, with transparency in data analyses and equity among collaborators to facilitate access and publication of relevant analyses. It is hoped that this APTAVI registry will set the template for more future collaboration in the region. Another project is the SYNERGY 3 Year Registry initiated by NUHCS, which will include nine centres from four Asian countries. It aims to examine the long-term safety and efficacy of everolimus-eluting platinum-chromium SYNERGY™ (Boston Scientific Corporation, Marlborough, MA, USA) stents over a three-year period.
Other important education activities include the designation of AsiaIntervention (https://www.asiaintervention.org) as the official journal of APSIC. First published in 2015, the journal hopes to boost clinical research and scientific communication within Asia and enhance the global visibility of research in this region. The journal is published twice a year and hopes to be PubMed listed soon. The revamp of the APSIC website (http://www.aspic.net) is another significant milestone. In this elegantly designed website, members will have the opportunity to access the latest up-to-date medical information as well as learn best practices from Asian experts for complex procedures.
On a personal note, I am happy to see the results of the training programme at NUHCS which I have set out to provide for the region. Of the more than 50 overseas interventional cardiology fellows trained since 2000 from AP, European and South American countries, many have emerged as prominent opinion leaders in their own countries and have grown to become experts of international repute (Figure 3, Figure 4). The PCI simulator course started in my centre for young aspiring fellows in 2006 has seen more than 300 participants go through simulator-based training; many are now established and competent interventionists. As I approach the end of my APSIC Presidency, I reflect with gratitude and view with great optimism and excitement the growth of endovascular therapy in the Asia-Pacific region. I deem myself fortunate to have experienced and contributed a small part to this growth journey. I continue to look forward to its future, one which is exceedingly promising and bright.
Conflict of interest statement
The authors have no conflicts of interest to declare.

Figure 3. Chinese NUH Alumni at Beijing CIT meeting 2019.

Figure 4. Filipino NUH Alumni at Manila PSCCI meeting 2019.
To download, please click below.