Gunasekaran Sengottuvelu*, MD, DM, FSCAI, FRCP; Paul Pandi Vinodh Kumar, MD, DM; Immaneni Sathyamurthy, MD, DM
AsiaIntervention 2019;5:132-133, DOI: 10.4244/AIJ-D-18-00033
Apollo Hospital, Chennai, Tamil Nadu, India
Coronary artery aneurysm (CAA) is defined as coronary dilatation which exceeds the diameter of normal adjacent segments or the diameter of the patient’s largest coronary vessel by 1.5 times1. The overall incidence of CAAs ranges from 1.5 to 5%, with a male preponderance and predilection for the right coronary artery1. We present a case report of iatrogenic CAAs which developed after Absorb™ bioresorbable vascular scaffold (BVS; Abbott Vascular, Santa Clara, CA, USA) implantation.
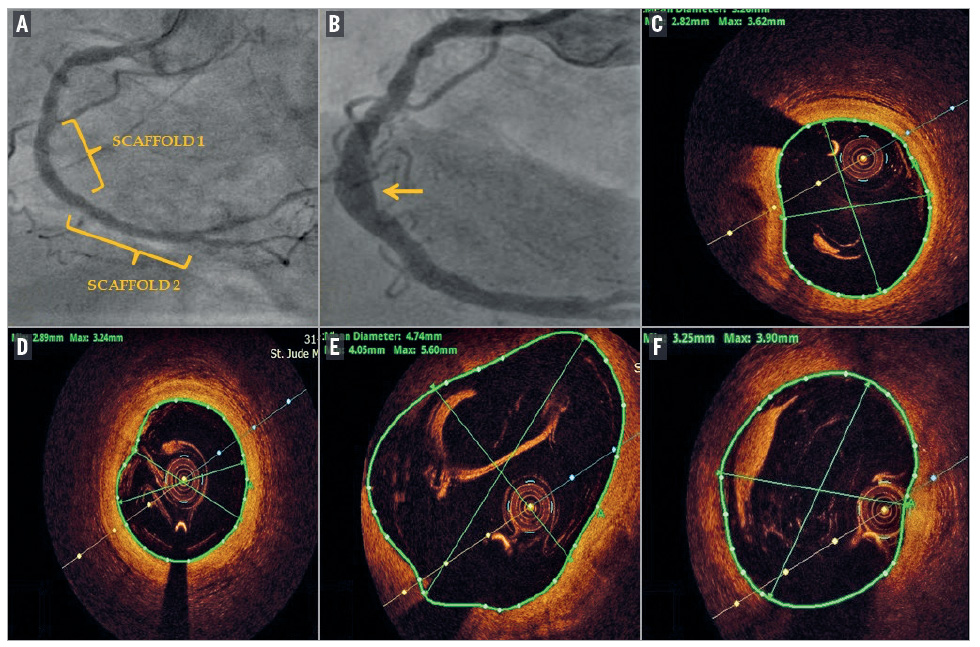
In 2013, a 65-year-old gentleman with hypertension, obesity, effort angina and positive stress test, underwent a coronary angiogram which revealed an occluded mid right coronary artery (RCA) and critical stenosis of the proximal left circumflex artery. Two overlapping Absorb BVS were deployed in the RCA (Panel A) and a staged PCI of the LCX with deployment of one Absorb BVS followed one month later. A coronary angiogram and OCT of the RCA were carried out five years later, as part of the study. This revealed an aneurysm in the mid RCA (Panel B, arrow) and LCX (Supplementary Figure 1). OCT showed complete resorption of the Absorb scaffold, with areas of near normal segments in the proximal RCA, having a maximum lumen diameter of 3.6 mm and lumen area of 8.4 mm² (Panel C). The mid RCA, after the aneurysmal segment, had a lumen diameter of 3.2 mm and area of 7.7 mm² (Panel D). There was a significant aneurysmal dilatation of the mid RCA with a maximum diameter of 5.6 mm (area 16.89 mm2) (Panel E). The distal RCA showed ectatic dilatation with an MLD of 3.9 mm (area 10.2 mm2) (Panel F).
In case reports, the time to aneurysm formation in BVS varies from 6 to 32 months. The reasons are not clear but could be due to aggressive bed preparation with resultant deep dissections. The distinct morphological characteristics of the BVS – thicker struts and slower expandability – require higher pressures for balloon inflation, which could damage the arterial wall2. Late development of scaffold strut discontinuity and the resultant outward displacement of struts may result in aneurysm formation. The polymer and the antiproliferative drug could also play a role3.
Conflict of interest statement
The authors have no conflicts of interest to declare.
References
1. Syed M, Lesch M. Coronary artery aneurysm: a review. Prog Cardiovasc Dis. 1997;40:77-84.
2. Varghese S, Lauer B, Ohlow MA. Coronary Artery Aneurysm After Everolimus-Eluting Bioabsorbable Vascular Scaffold Implantation. JACC Cardiovasc Interv. 2016;9:e23-5.
3. Abou Sherif S, Ozden Tok O, Taşköylü Ö, Goktekin O, Kilic ID. Coronary Artery Aneurysms: A Review of the Epidemiology, Pathophysiology, Diagnosis, and Treatment. Front Cardiovasc Med. 2017;4:24.
Supplementary data
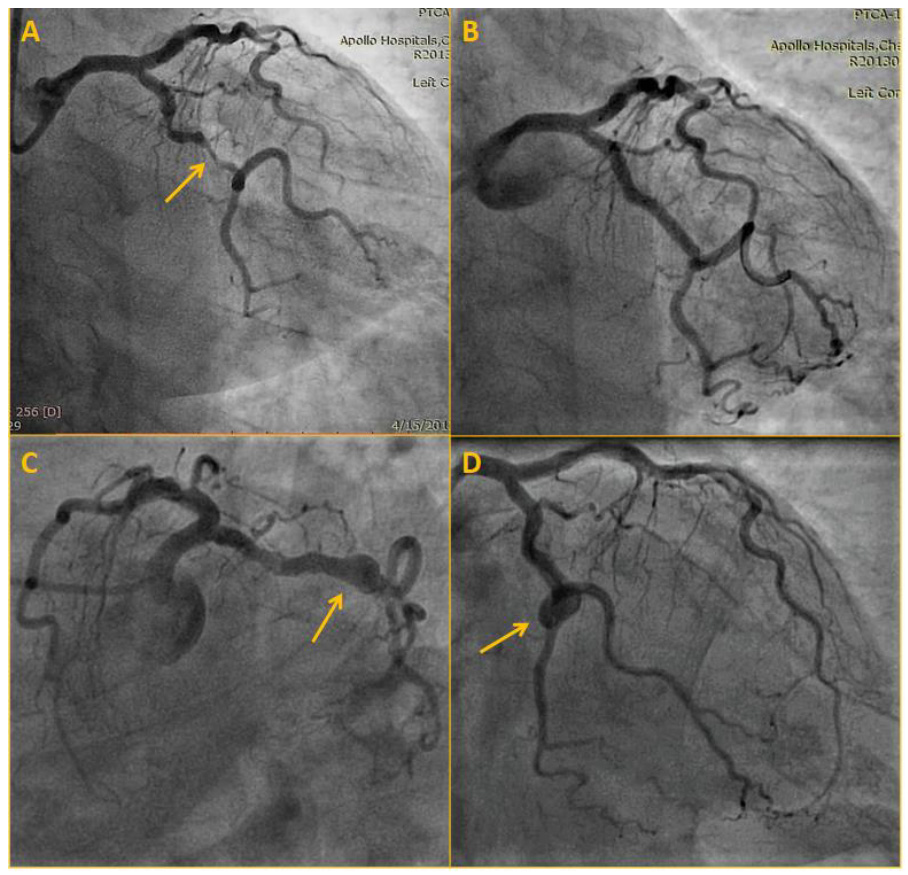
Supplementary Figure 1. Left circumflex artery angiogram at scaffold deployment and 5-year follow-up.
A) Significant stenosis of left circumflex artery (arrow).
B) Result after PCI indicating Absorb scaffold location.
C) & D) Follow-up angiogram after 5 years showing aneurysmal dilatation (arrow).
To download, please click below.