A 61-year-old hypertensive, non-diabetic, non-smoking male presented with rest angina in the emergency room. He had undergone percutaneous coronary intervention (PCI) of the mid-left anterior descending artery (LAD) with a 3.0×33 mm CYPHER stent (Cordis) deployment 15 years previously and a repeat PCI of mid-LAD late in-stent restenosis (ISR) with a 3.0×32 mm TAXUS stent (Boston Scientific) 3 years prior, at an outside hospital. His clinical examination was unremarkable. An electrocardiogram (ECG) showed right bundle branch block. An echocardiogram revealed a left ventricular ejection fraction of 45% and mild hypokinesia of the anterior wall. Coronary angiography revealed 90% diffuse ISR of the mid-LAD stent (Moving image 1). It was dilated with a 3.0×20 mm non-compliant balloon followed by a 3.0×15 mm WOLVERINE cutting balloon (Boston Scientific). Optical coherence tomography (OCT [St Jude/Abbott]) revealed homogeneous, diffuse intimal hyperplasia of the double-layered, underexpanded mid-LAD stented segment (Figure 1A, Moving image 2). It was further dilated with a 3.5×15 mm non-compliant balloon followed by a 4.0×30 mm paclitaxel-coated drug-eluting balloon (DEB; AGENT percutaneous transluminal coronary angioplasty balloon [Boston Scientific]). Angiography revealed no residual stenosis (Figure 1B). Repeat OCT revealed good luminal gain with a minimal lumen area of 4.99 mm2. It also showed multiple tiny, bright particles of approximately 10 μm in size adhered to the luminal surface of the arterial wall, suggestive of paclitaxel crystals from the DEB (Figure 1B, Moving image 3). These bright particles were not present in the OCT run before DEB inflation. The patient had an asymptomatic clinical follow-up of 4 months.
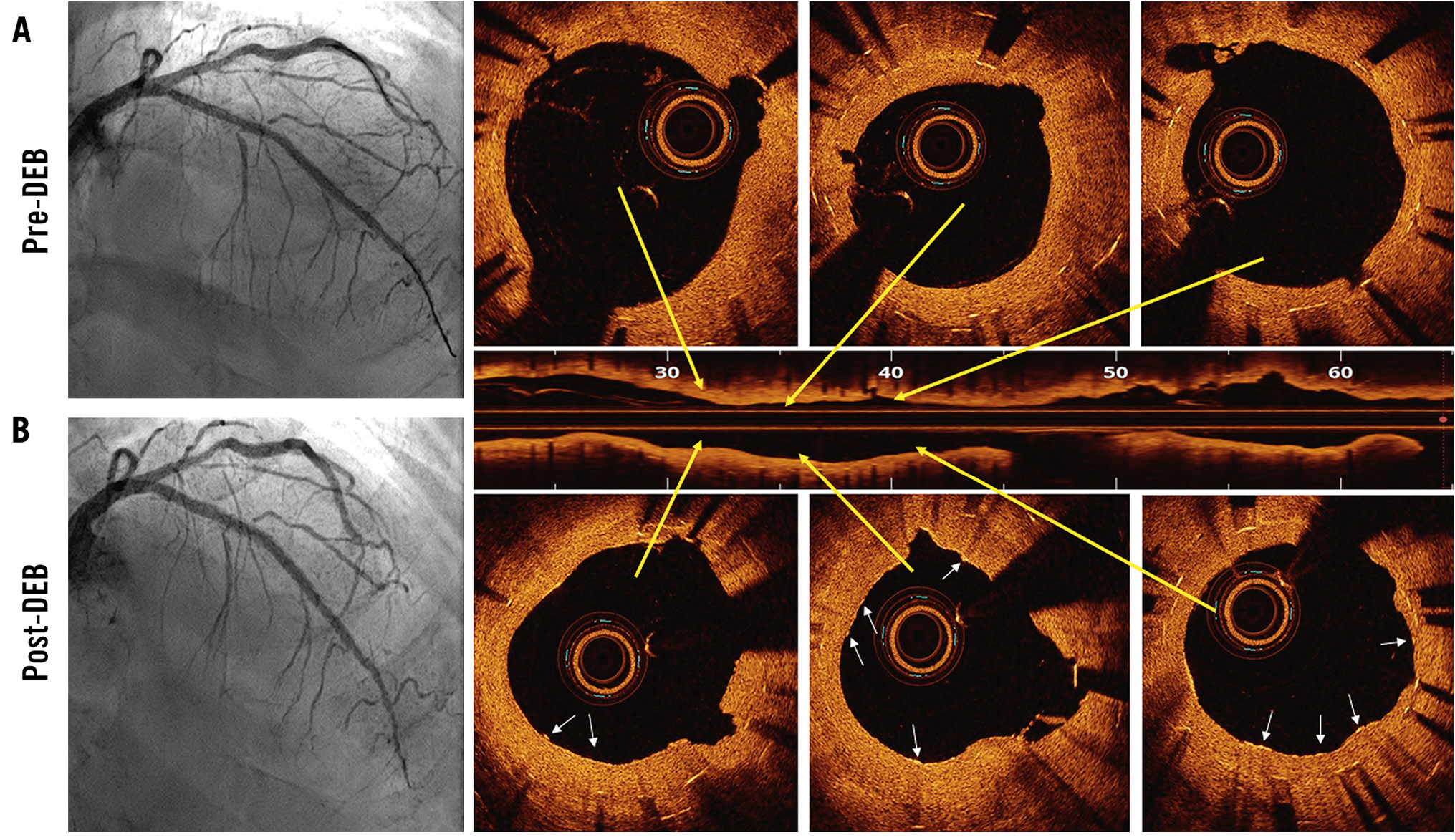
Figure 1. Optical coherence tomography (OCT) examination after balloon angioplasty of a mid-left anterior descending artery (LAD) in-stent restenosis (ISR) lesion. A) Angiographic luminal gain is shown following plain balloon angioplasty, and OCT shows homogeneous intimal hyperplasia along with two layers of underexpanded stents. B) The final angiographic outcome of the mid-LAD ISR lesion is shown, and OCT shows good luminal gain and visualisation of multiple tiny, bright paclitaxel crystals (white arrows) adhered to the endoluminal surface of the arterial wall.
Conflict of interest statement
The authors have no conflicts of interest regarding the present study to declare.
