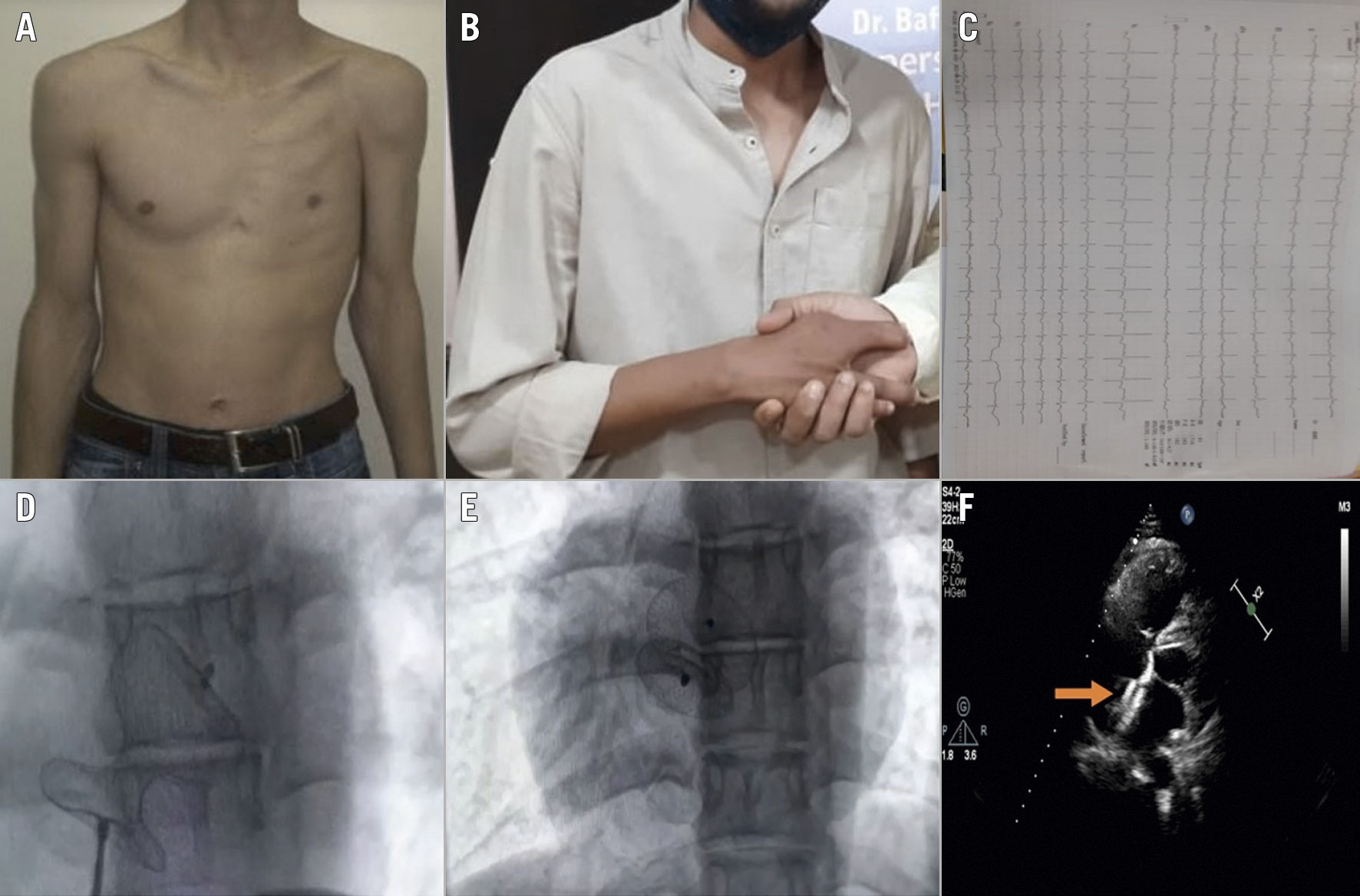
Figure 1. Percutaneous atrial septal defect closure in a case of Poland syndrome with dextrocardia. A. Physical examination showing depression of the left anterior chest wall. B. Patient’s right hand with bilateral syndactyly of second and third fingers. C. Electrocardiogram showing within normal limit. D. Fluoroscopic image showing loaded Amplatzer Occluder. E. Fluoroscopic image showing appropriate positioning of Amplatzer ASD closure device. F. Transthoracic echocardiography confirmed the appropriate positioning of Amplatzer ASD closure device.
A 16-year-old male presented complaining that for six months he had suffered dyspnoea on exertion and easy fatigability. A physical examination showed depression of the left anterior chest wall (Figure 1A), cardiac apex at the fifth right intercostal space below the nipple, and bilateral syndactyly of second and third fingers of his right hand (Figure 1B). A radiological examination revealed the absence of the major pectoralis muscle on the left side and mirror-image dextrocardia. The second heart sound was noted fixed and widely split. His vital signs were within normal range and the electrocardiogram (Figure 1C) examination was unremarkable. He was haemodynamically stable with normal peripheral pulse and 98% SpO2. An echocardiogram revealed a 22 mm secundum atrial septal defect (ASD) leading to significant left-to-right shunting. The diagnosis was a rare case of Poland syndrome and dextrocardia with ASD.
Percutaneous closure of ASD was performed the next day through the right femoral vein under local anaesthesia. The right femoral vein was accessed and a 6 Fr Judkins right catheter (JR) was advanced through the inferior vena cava, followed by the right and left atrium over a 0.035″ double length J-tip wire (Translumina Therapeutics). The 6 Fr JR was exchanged for a 0.035″ DL J-Tip Amplatz Super Stiff wire (Boston Scientific). The wire tip was positioned in the left superior pulmonary vein. A 12 Fr Amplatzer ASD Occluder (Abbott) delivery sheath was used with a (145°) distal curve. A 28 mm Amplatzer Occluder was loaded and advanced through the sheath (Figure 1D). The occluder disc was deployed in the left atrium, and the system was pulled until the disc for the left atrium was against the septum. Thereafter, the disc for the right atrium was deployed and placed at the right atrium septum. The position of the ASD closure device was confirmed by transoesophageal and transthoracic echocardiography and fluoroscopy (Figure 1E, Figure 1F), and the ASD device was disengaged from its introducer assembly (Moving image 1). The intervention was completed successfully, and the further course was uneventful. An echocardiographic study showed no residual shunting (Moving image 2). An anticoagulation protocol was followed before and during the intervention as well as postoperatively. In dextrocardia, the interatrial septum is directed anteriorly, malpositioned, and challenging to access compared to normal cardiac ASD. The technical difficulties encountered during device closure of ASD in dextrocardia required skilful interventionists, appropriate planning, and the use of imaging technologies for patient safety and a successful intervention.
Conflict of interest statement
The authors have no conflicts of interest to declare.
