Akihisa Kataoka*, MD, PhD; Yusuke Watanabe, MD, PhD; Makoto Nakashima, MD; Ken Kozuma, MD, PhD
AsiaIntervention 2019;5:68-69, DOI: 10.4244/AIJ-D-18-00007
Department of Medicine, Division of Cardiology, Teikyo University, Tokyo, Japan
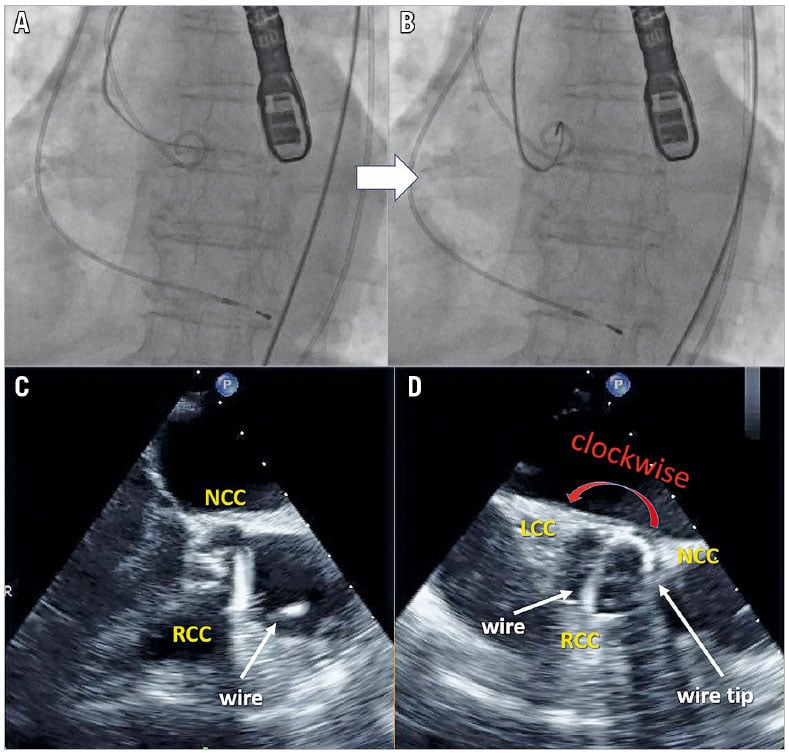
A 90-year-old woman, with severe calcific aortic stenosis (maximum velocity 4.9 m/sec, mean pressure gradient 58 mmHg, and aortic valve area 0.43 cm2), underwent transfemoral transcatheter aortic valve replacement (TAVR) using general anaesthesia and transoesophageal echocardiography (TOE), IE-33 (Philips Medical Systems, Andover, MA, USA) with an X7-2t matrix transducer, which can visualise the aortic valve (AV) simultaneously in the long and short axes1. We encountered difficulty crossing the stenosed AV with the tip of the catheter, which was slightly close to the AV (Panel A, Panel B, Moving image 1). The live X-plane mode of the TOE showed that the tip of the wire was located and trapped on the non-coronary cusp (Panel C, Panel D, Moving image 2). Based on the echocardiologist’s suggestion, the interventionist moved the wire clockwise and pulled the Judkins right catheter slightly, so that it could be relocated between the noncoronary and left coronary cusps, resulting in crossing of the wire. This case shows the crossing of a TOE-guided wire in a stenosed AV during TAVR. We achieved crossing by running the wire between the non-coronary cusp and the left coronary cusp. Obtaining detailed assessment of wire location and direction is difficult using a fluoroscope only; frequent wire adjustment increases the risk of cerebral embolism substantially2. This simple and easy technique can decrease risk in patients, decrease radiation exposure and save time.
Conflict of interest statement
The authors have no conflicts of interest to declare.
References
1. McGhie JS, de Groot-de Laat L, Ren B, Vletter W, Frowijn R, Oei F, Geleijnse ML. Transthoracic two-dimensional xPlane and three-dimensional echocardiographic analysis of the site of mitral valve prolapse. Int J Cardiovasc Imaging. 2015;31:1553-60.
2. Omran H, Schmidt H, Hackenbroch M, Illien S, Bernhardt P, von der Recke G, Fimmers R, Flacke S, Layer G, Pohl C, Lüderitz B. Silent and apparent cerebral embolism after retrograde catheterisation of the aortic valve in valvular stenosis: a prospective, randomised study. Lancet. 2003;361:1241-6.
Supplementary data
Moving image 1. Failure of wire crossing to the aortic valve under a fluoroscope.
Moving image 2. Failure of wire crossing to the aortic valve in live X-plane transoesophageal echocardiography mode.
To download, please click below.